DKA vs HHS: critical care nurse's guide to diagnosis
![]()
TL;DR:
- DKA and HHS are distinct hyperglycemic emergencies with different pathophysiology, labs, and treatment protocols. Recognizing their differences is vital for safe management and exam success, especially given the rising prevalence of overlap syndrome and SGLT2 inhibitor-related euglycemic DKA. Mastery of their nuances enhances clinical judgment, minimizes errors, and improves patient outcomes.
DKA vs HHS is one of the highest-yield comparisons on the CCRN exam, and it’s also one of the most mismanaged conditions at the bedside. These two diabetic emergencies look similar on the surface but differ sharply in pathophysiology, lab findings, and treatment priorities. Get the distinction wrong in clinical practice and you risk cerebral edema, fatal arrhythmias, or delayed insulin therapy. Get it wrong on the exam and you lose points on questions that should be automatic. This guide gives you the clinical depth to confidently handle both.
Table of Contents
- Understanding the pathophysiology and epidemiology of DKA and HHS
- Key clinical and laboratory differences: diagnosing DKA vs HHS
- Tailoring treatment: management principles for DKA, HHS, and overlap syndrome
- Emerging challenges: overlap syndrome and impact of SGLT2 inhibitors
- Summary tables and nursing considerations for CCRN exam prep and clinical care
- Why mastering DKA vs HHS nuances can be a game changer for critical care nurses
- Boost your CCRN success with targeted practice on endocrine emergencies
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Differentiate dka and hhs | DKA features acidosis and ketosis with moderate hyperglycemia, while HHS has extreme hyperglycemia and hyperosmolality without significant ketosis. |
| Overlap syndrome risk | Mixed DKA-HHS presentations increase mortality risk and require tailored management. |
| Insulin timing with potassium | Delay insulin until serum potassium exceeds 3.3 mEq/L to prevent fatal hypokalemia. |
| Fluid management nuances | HHS needs cautious fluid correction to avoid osmotic brain injury, unlike the more rapid rehydration in DKA. |
| SGLT2 inhibitors complicate diagnosis | These drugs can cause euglycemic DKA, requiring ketone and acid-base testing despite normal glucose. |
Understanding the pathophysiology and epidemiology of DKA and HHS
DKA and HHS sit on the same spectrum of hyperglycemic crisis, but they represent different failure points in insulin physiology. In DKA, absolute insulin deficiency triggers unopposed glucagon activity, which accelerates lipolysis and floods the liver with free fatty acids. The result is ketone body production, metabolic acidosis, and a pH that can drop below 7.1 in severe cases. The insulin deficiency spectrum is the key concept here: DKA is the extreme low end.
HHS involves relative, not absolute, insulin deficiency. There is just enough circulating insulin to suppress ketogenesis, but not enough to control glucose. The result is extreme hyperglycemia, sometimes exceeding 1,000 mg/dL, combined with massive osmotic diuresis and profound dehydration. Fluid deficits in HHS can reach 8 to 10 liters, compared to 3 to 6 liters in DKA.
Understanding the DKA vs HHS differences in patient population matters clinically and for exam context:
- DKA most often affects patients with type 1 diabetes, though it occurs in type 2 as well. Two-thirds of adult DKA cases occur in type 1 diabetes, while 90% of HHS cases occur in type 2 diabetes.
- HHS typically affects older adults with type 2 diabetes, often with a precipitating illness like infection, stroke, or MI.
- DKA mortality is approximately 1 to 2%, while HHS mortality reaches 10 to 20%, largely because of the older, more comorbid patient population.
- Overlap syndrome, where both conditions coexist, is increasingly recognized and carries the worst prognosis of all three presentations.
The mortality gap between DKA and HHS is not just a trivia fact for the exam. It shapes how urgently you act, how aggressively you monitor, and how carefully you correct fluid deficits.
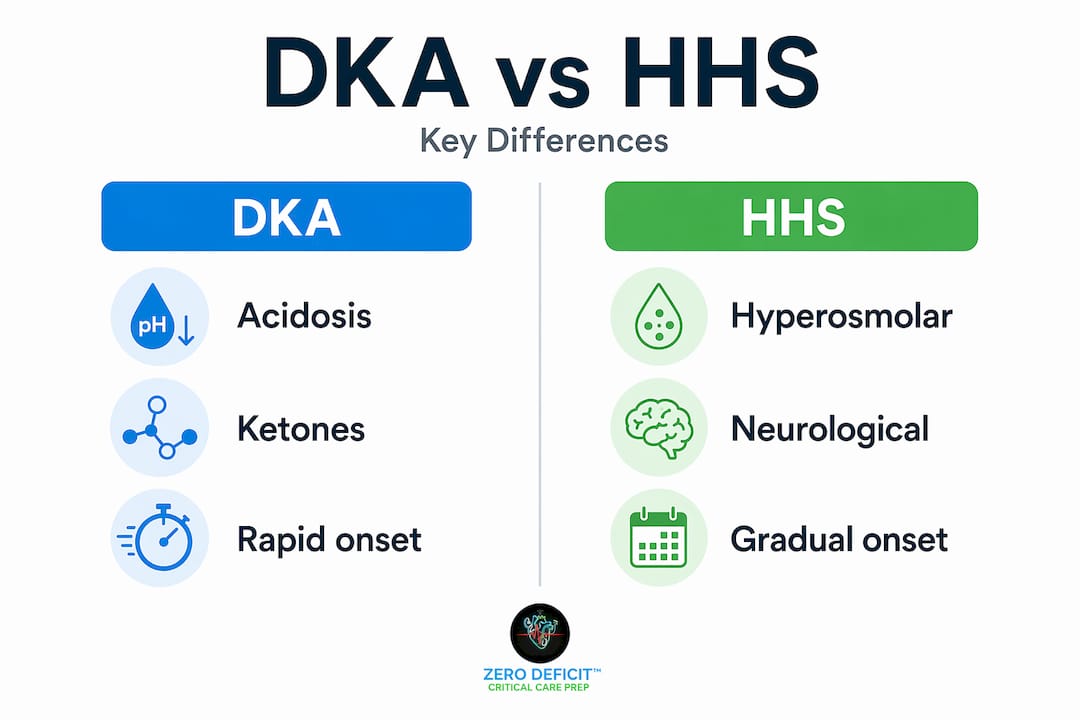
Key clinical and laboratory differences: diagnosing DKA vs HHS
The symptoms of DKA and HHS reflect their underlying physiology. DKA develops over hours to a day or two. Patients present with nausea, vomiting, abdominal pain, Kussmaul respirations (deep, rapid breathing to blow off CO2), and a fruity odor from acetone. Mental status is often preserved or only mildly altered.
HHS develops over days to weeks. The presenting symptom is usually profound neurological impairment, ranging from confusion to frank coma, driven by hyperosmolality rather than acidosis. The neurologic symptoms in hyperglycemic emergencies are a direct function of serum osmolality. When osmolality exceeds 320 mOsm/kg, cognitive dysfunction begins. Above 340 mOsm/kg, coma is common.
Here is the comparison you need to know cold:
| Parameter | DKA | HHS |
|---|---|---|
| Blood glucose | ≥200 mg/dL | >600 mg/dL |
| Serum pH | <7.3 | ≥7.3 |
| Bicarbonate | <18 mmol/L | ≥15 to 18 mmol/L |
| β-hydroxybutyrate | ≥3.0 mmol/L | <3 mmol/L |
| Serum osmolality | Variable | >320 mOsm/kg |
| Ketones | Significant | Minimal or absent |
| Onset | Hours to 1 to 2 days | Days to weeks |
| Mental status | Alert to mildly altered | Confusion to coma |
| Typical diabetes type | Type 1 (mostly) | Type 2 (mostly) |
The diagnostic criteria for DKA and HHS are well established: DKA requires glucose ≥200 mg/dL, β-hydroxybutyrate ≥3.0 mmol/L, pH <7.3, and bicarbonate <18 mmol/L. HHS is defined by glucose >600 mg/dL, osmolality >320 mOsm/kg, pH ≥7.3, and minimal ketones.
Key clinical flags to watch for:
- Kussmaul breathing and fruity breath point to DKA, not HHS.
- Focal neurological deficits in HHS can mimic stroke.
- Abdominal pain in DKA can mimic a surgical abdomen. If it persists after glucose correction, investigate further.
- Overlap syndrome: suspect it when glucose is markedly elevated AND ketones AND acidosis are all present together.
Pro Tip: Always calculate effective osmolality in any hyperglycemic emergency. The formula is 2(Na) + glucose/18. If it is above 320 mOsm/kg with altered mental status, HHS or overlap syndrome is on the table regardless of what the glucose alone looks like.
Tailoring treatment: management principles for DKA, HHS, and overlap syndrome
The treatment for DKA and HHS shares common elements but differs in critical ways. Applying the wrong protocol to the wrong condition can be fatal.
For DKA, follow this sequence:
- Start IV fluids immediately: 1 liter of 0.9% normal saline over the first hour.
- Check serum potassium before touching insulin.
- If potassium is below 3.3 mEq/L, hold insulin and replace potassium at 20 to 40 mEq/h until K+ exceeds 3.3 mEq/L.
- Start insulin infusion at 0.1 units/kg/h once potassium is adequate.
- When glucose reaches 200 mg/dL, switch fluids to dextrose-containing solution and reduce insulin to 0.02 to 0.05 units/kg/h.
- Resolution criteria: pH >7.3, bicarbonate ≥15 mmol/L, anion gap ≤12 mEq/L.
For HHS:
- Fluids are the primary treatment. HHS treatment prioritizes fluids first, with insulin at 0.05 units/kg/h only if glucose fails to fall adequately with fluids alone.
- Correct fluid deficits slowly, over 24 to 48 hours, to prevent cerebral edema.
- Resolution target: osmolality below 300 mOsm/kg with restored mental status.
- Monitor potassium just as closely as in DKA. Osmotic diuresis depletes it.
For fluid and electrolyte management in DKA and HHS, the approach hinges on volume status monitoring throughout the resuscitation.
Key electrolyte considerations for both conditions:
- Potassium: Replace aggressively. Target 4 to 5 mEq/L during treatment.
- Phosphate: Replace if below 1.0 mg/dL or if patient has cardiac or respiratory dysfunction.
- Sodium: Watch for pseudohyponatremia. Correct measured sodium by adding 1.6 mEq/L for every 100 mg/dL glucose above 100.
Pro Tip: In overlap syndrome, you need to address both the anion gap acidosis and the hyperosmolality simultaneously. Start fluids as in HHS, but do not delay insulin as long as potassium allows. Recheck labs every 2 hours and adjust based on the slower-resolving abnormality.
Emerging challenges: overlap syndrome and impact of SGLT2 inhibitors
Overlap syndrome is no longer a rare edge case. Overlap syndrome carries a higher mortality around 8% compared to isolated DKA or HHS, and its incidence is rising as the type 2 diabetes population grows and ages. These patients have both significant ketoacidosis and extreme hyperglycemia with hyperosmolality, meaning you cannot treat them purely by either protocol.
The other challenge reshaping insulin deficiency spectrum and DKA-HHS overlap presentations is the widespread use of SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin). These medications increase glucose excretion in the urine, which means patients on them can develop DKA with glucose levels that are only mildly elevated, sometimes under 250 mg/dL. This is called euglycemic DKA.
Euglycemic DKA is a diagnostic trap. The glucose is not dramatically elevated, so the clinical picture looks less urgent. But the acidosis and ketosis are real and dangerous. If you are not checking ketones and pH in every patient on an SGLT2 inhibitor who presents with nausea, fatigue, or vomiting, you will miss it.
Key points on SGLT2 inhibitor-related DKA:
- Precipitants include infection, surgery, fasting, reduced insulin doses, and alcohol use.
- Treatment follows standard DKA protocol, but glucose targets need adjustment since the patient is not markedly hyperglycemic.
- Patient education on sick-day rules and when to hold SGLT2 inhibitors is a primary prevention strategy.
- Always check a urine or serum ketone level in any patient on these medications presenting with metabolic symptoms, even if glucose appears near-normal.
Pro Tip: When a patient on an SGLT2 inhibitor has an anion gap metabolic acidosis and no obvious cause, euglycemic DKA is your diagnosis until proven otherwise. Do not let a glucose of 180 mg/dL falsely reassure you.
Summary tables and nursing considerations for CCRN exam prep and clinical care
The diagnostic and management framework for DKA and HHS is best retained when you can visualize it at a glance. Use this as your quick-reference summary:
| Feature | DKA | HHS | Overlap |
|---|---|---|---|
| Glucose | ≥200 mg/dL | >600 mg/dL | >600 mg/dL |
| pH | <7.3 | ≥7.3 | <7.3 |
| Bicarb | <18 mmol/L | ≥15 to 18 mmol/L | <18 mmol/L |
| Ketones | Significant | Minimal | Significant |
| Osmolality | Variable | >320 mOsm/kg | >320 mOsm/kg |
| Fluid deficit | 3 to 6 L | 8 to 10 L | 6 to 10 L |
| Insulin start | After K+ >3.3 | After fluids | After K+ and fluids |
| Mortality | ~1 to 2% | ~10 to 20% | ~8% |
Nursing priorities during active treatment:
- Check glucose every hour during insulin infusion.
- Check electrolytes (especially potassium) every 2 hours for the first 6 hours.
- Monitor urine output as a proxy for volume status and renal perfusion.
- Assess neurological status frequently in HHS. Rapid osmolality correction can cause cerebral edema.
- Document anion gap at each lab draw in DKA to track resolution.
- Watch for signs of fluid overload, especially in older HHS patients with cardiac history.
These CCRN exam study tips apply directly here: use the table above to practice elimination strategies on exam questions. If a question describes Kussmaul breathing with glucose of 280 mg/dL, that is DKA. If it describes an 80-year-old with a glucose of 900 mg/dL and no respiratory changes, that is HHS. The lab pattern tells the story.
Pro Tip: On the CCRN exam, the question stem will often test whether you know the correct sequence of interventions. Insulin before checking potassium in DKA is a wrong answer every time. Fluids before insulin in HHS is always right.
Why mastering DKA vs HHS nuances can be a game changer for critical care nurses
Most nurses learn DKA and HHS as two separate boxes with a checklist for each. That works for straightforward presentations. It fails for the patients who are actually in front of you at 2 AM with glucose of 750 mg/dL, a pH of 7.25, and an osmolality of 335 mOsm/kg. That patient does not fit either box cleanly, and a rigid protocol approach will hurt them.
The real skill is understanding the underlying physiology well enough to reason through the overlap. When you know why insulin drives potassium intracellularly, you do not need to memorize the rule. You understand it. When you know why rapid fluid correction in HHS risks cerebral edema, you pace your resuscitation with intention rather than anxiety. That depth of insulin deficiency insights is what separates nurses who manage these patients confidently from those who are just executing orders.
For the CCRN exam, understanding DKA and HHS at this level is a genuine advantage. These conditions appear across multiple body system categories, including endocrine, renal, and neurological. A nurse who understands the osmolality formula, the anion gap, and the potassium-insulin relationship can answer questions from any angle. A nurse who memorized a table can only answer the ones that look exactly like the table.
This is also a high-stakes area for patient safety. The errors that kill patients in DKA and HHS are not rare or exotic. They are insulin given before potassium is checked, fluids corrected too fast in HHS, and euglycemic DKA missed because glucose looked normal. Mastery here is not academic. It is directly protective.
Boost your CCRN success with targeted practice on endocrine emergencies
Understanding DKA and HHS at a clinical level is the foundation. Testing that understanding under exam conditions is what builds the confidence to pass. Zero Deficit™ CCRN Prep gives you both. Our comprehensive CCRN study guides cover endocrine emergencies with the same depth you just read, organized by body system so your review stays focused and efficient.
When you are ready to test your knowledge, our CCRN practice questions put DKA, HHS, and overlap syndrome scenarios in front of you the way the actual exam does, with detailed rationales that reinforce the why behind every answer. You can also explore high-yield CCRN topics to identify where your gaps are before exam day. No credit card required to start. Just focused, effective prep built for critical care nurses who are serious about passing the first time.
Frequently asked questions
What are the main lab values that differentiate DKA from HHS?
DKA is diagnosed by glucose ≥200 mg/dL, β-hydroxybutyrate ≥3.0 mmol/L, pH <7.3, and bicarbonate <18 mmol/L, while HHS presents with glucose >600 mg/dL, osmolality >320 mOsm/kg, pH ≥7.3, and minimal ketones below 3 mmol/L. The presence of significant ketosis and acidosis is the clearest separator between the two.
Why must insulin be delayed in DKA if potassium is low?
Insulin drives potassium into cells, which can worsen existing hypokalemia and trigger fatal cardiac arrhythmias. Per established DKA insulin guidelines, insulin should start only after potassium exceeds 3.3 mEq/L, with replacement running at 20 to 40 mEq/h if needed, and potassium rechecked every 2 hours during the infusion targeting 4 to 5 mEq/L.
What unique challenges does the DKA-HHS overlap syndrome present?
Overlap syndrome combines metabolic acidosis with extreme hyperglycemia and hyperosmolality, creating increased risks of cerebral edema, thromboembolism, and acute kidney injury, with mortality around 8%. Management requires balancing aggressive fluid resuscitation against the risk of rapid osmolality shifts while simultaneously addressing the anion gap acidosis.
How do SGLT2 inhibitors affect DKA presentations?
SGLT2 inhibitors increase euglycemic DKA risk, producing metabolic acidosis and ketosis without marked hyperglycemia, which delays recognition and treatment. Always check ketones and acid-base status in any patient on these medications who presents with metabolic symptoms, even when glucose appears near-normal.
What is the correct fluid strategy in HHS versus DKA?
In DKA, begin with 1 liter of 0.9% normal saline in the first hour, then adjust based on corrected sodium and hemodynamic status. In HHS, fluid deficits are larger (8 to 10 liters) and must be corrected slowly over 24 to 48 hours to prevent cerebral edema, making pacing and frequent neurological reassessment critical throughout resuscitation.
Recommended
Take a Endocrine practice quiz
Test your DKA, HHS, thyroid storm, and adrenal crisis knowledge.
Ready to pass your CCRN?
Join 12,000+ nurses using Zero Deficit — 695+ practice questions with rationales, AI-powered weak-area drilling, and spaced-repetition flashcards.
Start Free Trial →